


 Sign Out
Sign Out


The safety of BRILINTA in patients with acute coronary syndromes (UA, NSTEMI and STEMI) was evaluated in the PLATO Study, which compared patients treated with BRILINTA 90 mg twice daily to patients treated with clopidogrel 75 mg once daily both given in combination with ASA and other standard therapies. Median treatment duration for BRILINTA was 277 days. In PLATO, patients on BRILINTA had a higher incidence of discontinuation due to adverse events than clopidogrel (7.4% vs. 5.4%).
The safety of BRILINTA in patients with history of MI (MI occurred at least one year ago) and high risk of developing a thrombotic event was evaluated in the PEGASUS Study, which compared patients treated with BRILINTA 60 mg twice daily or 90 mg twice daily combined with ASA to ASA therapy alone and other standard therapies. Median treatment duration for BRILINTA 60 mg was 29.4 months. In PEGASUS, patients on BRILINTA had a higher incidence of discontinuation due to adverse events compared to ASA therapy alone (16.1% for ticagrelor 60 mg with ASA vs. 8.5% for ASA therapy alone).
The most commonly reported adverse drug reactions in patients treated with ticagrelor were bleeding and dyspnoea (see also Precautions).
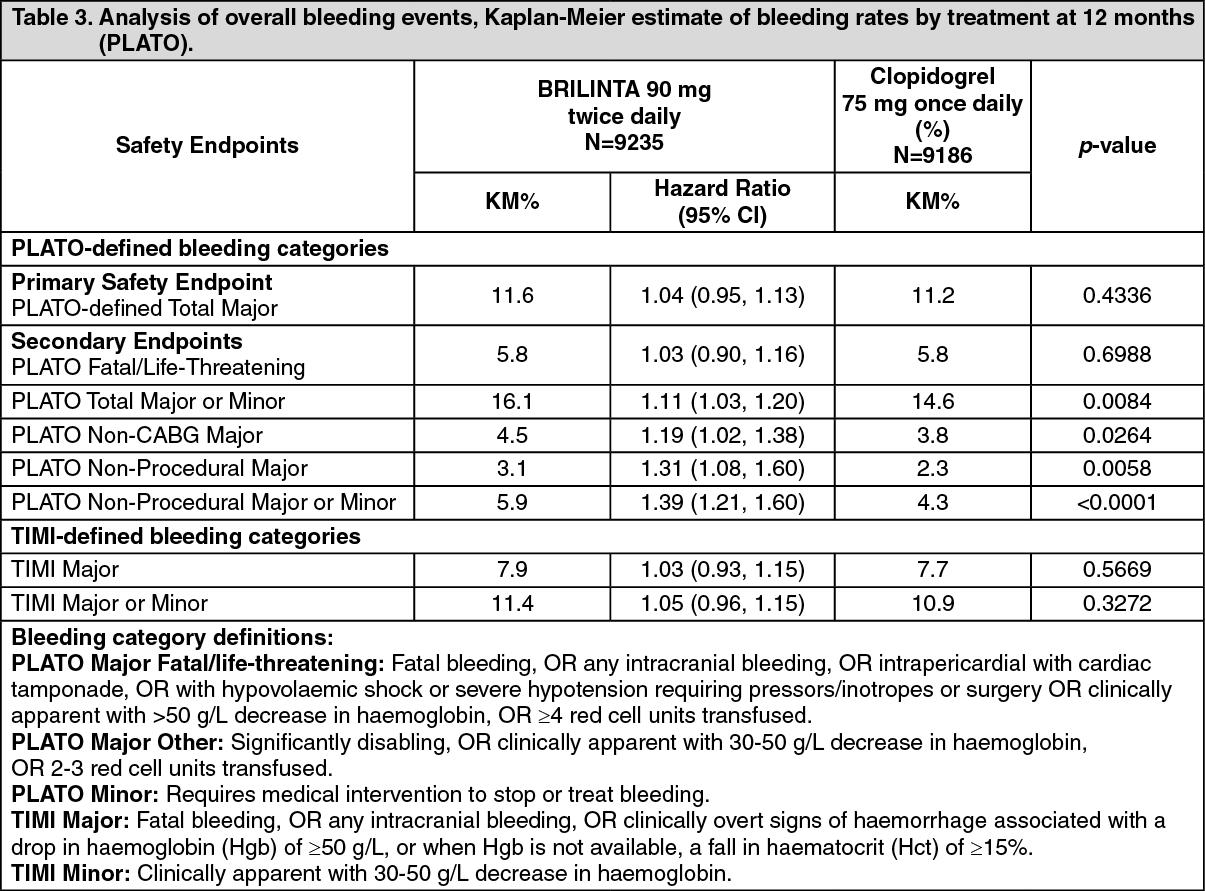
Description of selected adverse drug reactions: Bleeding findings in PLATO: Overall outcome of bleeding events in the PLATO Study are shown in Table 3. (See Table 3.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageIn PLATO, time to first PLATO-defined Total Major bleeding for BRILINTA did not differ significantly from that of clopidogrel. There were few fatal bleeding events in the study, 20 (0.2%) for BRILINTA 90 mg twice daily and 23 (0.3%) for clopidogrel 75 mg once daily. When minor bleeding was included, combined PLATO-defined Major and Minor bleeding events were significantly higher on BRILINTA than on clopidogrel. Overall rates of TIMI-defined bleeding events did not differ significantly between BRILINTA and clopidogrel.
CABG-related bleeding: In PLATO, 42% of the 1584 patients (12% of cohort) who underwent CABG surgery had a PLATO-defined Major Fatal/Life-threatening bleeding with no difference between the treatment groups. Fatal CABG bleeding occurred in 6 patients in each treatment group (see Precautions).
Non-CABG related bleeding and non-procedural related bleeding: BRILINTA and clopidogrel did not differ in non-CABG PLATO-defined Major Fatal/Life-threatening bleeding, but PLATO-defined Total Major, TIMI Major, and TIMI Major + Minor bleeding were more common with ticagrelor. Similarly, when removing all procedure related bleeding, more bleeding occurred with ticagrelor than with clopidogrel (Table 3). Discontinuation of treatment due to non-procedural bleeding was more common for ticagrelor (2.9%) than for clopidogrel (1.2%; p<0.001).
Age, gender, weight, ethnicity, geographic region, concurrent conditions, concomitant therapy and medical history, including a previous stroke or transient ischaemic attack, all did not predict either overall or non-procedural PLATO-defined Major bleeding. Thus no particular risk group was identified at risk for any subset of bleeding.
Intracranial bleeding: There were more intracranial non-procedural bleeds with ticagrelor (n=27 bleeds in 26 patients, 0.3%) than with clopidogrel (n=14 bleeds, 0.2%), of which 11 bleeds with ticagrelor and 1 with clopidogrel were fatal. There was no difference in overall fatal bleeds. The percentage of intracranial bleeding was low in both treatment groups given the significant comorbidity and cardiovascular risk factors of the population under study.
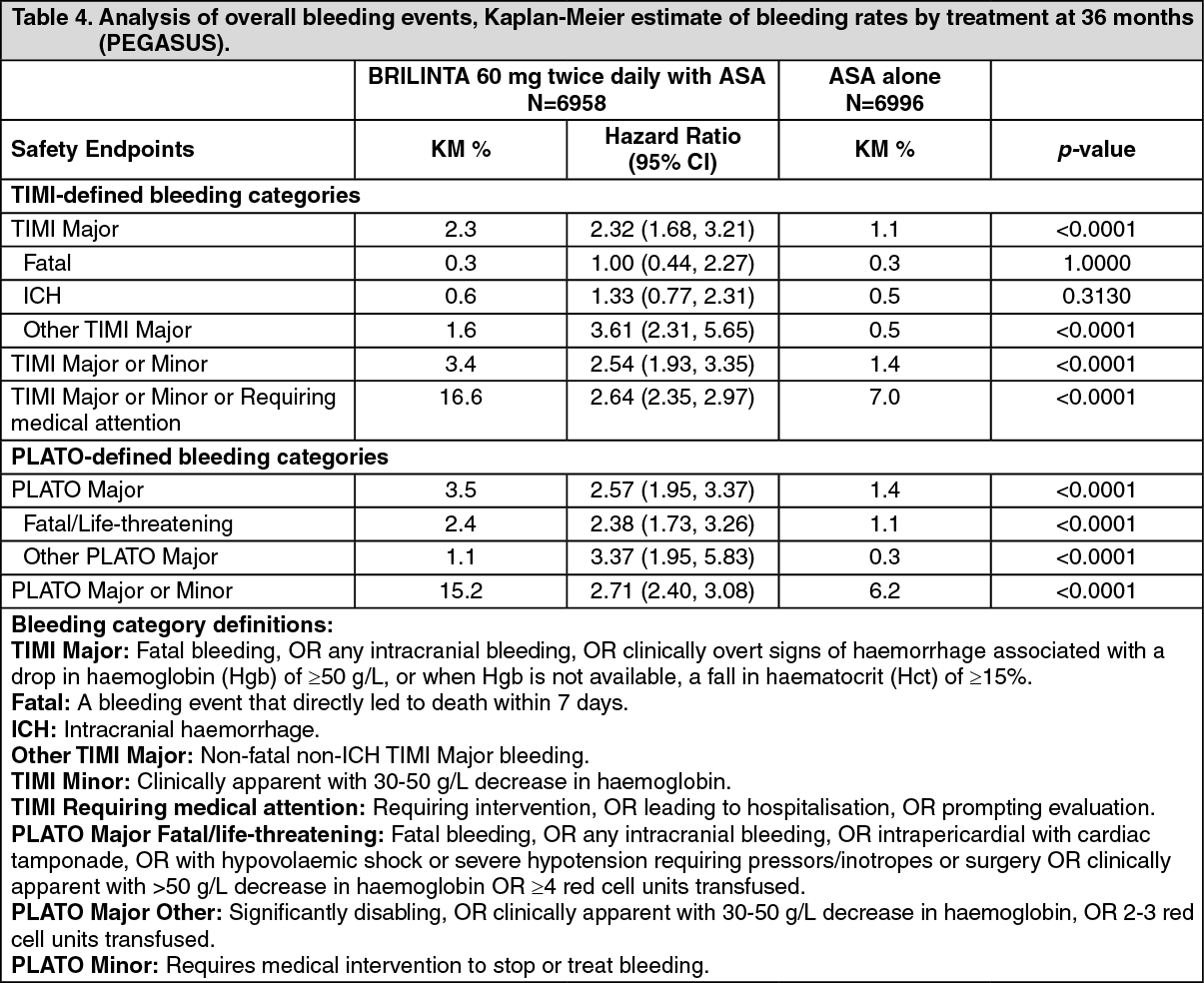
Bleeding findings in PEGASUS: Overall outcome of bleeding events in the PEGASUS Study are shown in Table 4. (See Table 4.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageIn PEGASUS, TIMI Major bleeding for BRILINTA 60 mg twice daily was higher than for ASA alone. No increased bleeding risk was seen for fatal bleeding and only a minor increase was observed in intracranial haemorrhages, as compared to ASA therapy alone. There were few fatal bleeding events in the study, 11 (0.3%) for BRILINTA 60 mg and 12 (0.3%) for ASA therapy alone. The observed increased risk of TIMI Major bleeding with BRILINTA 60 mg was primarily due to a higher frequency of Other TIMI Major bleeding driven by events in the gastrointestinal SOC.
Increased bleeding patterns similar to TIMI Major were seen for TIMI Major or Minor and PLATO-defined Major and PLATO-defined Major or Minor bleeding categories (see Table 4). Discontinuation of treatment due to bleeding was more common with BRILINTA 60 mg compared to ASA therapy alone (6.2% and 1.5%, respectively). The majority of these bleedings were of less severity (classified as TIMI Requiring medical attention), e.g. epistaxis, bruising, and haematomas.
The bleeding profile of BRILINTA 60 mg was consistent across multiple pre-defined subgroups (e.g. by age, gender, weight, race, geographic region, concurrent conditions, concomitant therapy, and medical history) for TIMI Major, TIMI Major or Minor, and PLATO-defined Major bleeding events.
Intracranial bleeding: Spontaneous ICHs were reported in similar rates for BRILINTA 60 mg and ASA therapy alone (n=13, 0.2% in both treatment groups). Traumatic and procedural ICHs showed a minor increase with BRILINTA 60 mg treatment, (n=15, 0.2%) compared with ASA therapy alone (n=10, 0.1%). There were 6 fatal ICHs with BRILINTA 60 mg and 5 fatal ICHs with ASA therapy alone. The incidence of intracranial bleeding was low in both treatment groups given the significant comorbidity and cardiovascular risk factors of the population under study.
Dyspnoea: In PLATO, dyspnoea adverse events were reported in 13.8% of patients taking ticagrelor 90 mg twice daily and in 7.8% of patients taking clopidogrel 75 mg once daily. Most reported dyspnoea adverse events were mild to moderate in intensity and often resolved without the need of treatment discontinuation. Dyspnoea was usually reported in the initial phase of treatment and 87% of the patients who reported dyspnoea experienced a single episode. Dyspnoea serious adverse events were reported in 0.7% taking ticagrelor and 0.4% taking clopidogrel. Patients who reported dyspnoea tended to be older and more frequently had dyspnoea, CHF, COPD, or asthma at baseline. PLATO data do not suggest that the higher frequency with BRILINTA is due to new or worsening heart or lung disease. There was no indication of an adverse effect of BRILINTA on pulmonary function (see Precautions).
In PEGASUS, dyspnoea was reported in 14.2% of patients taking BRILINTA 60 mg twice daily and in 5.5% of patients taking ASA alone. As in PLATO, most reported dyspnoea was mild to moderate in intensity (see Precautions).
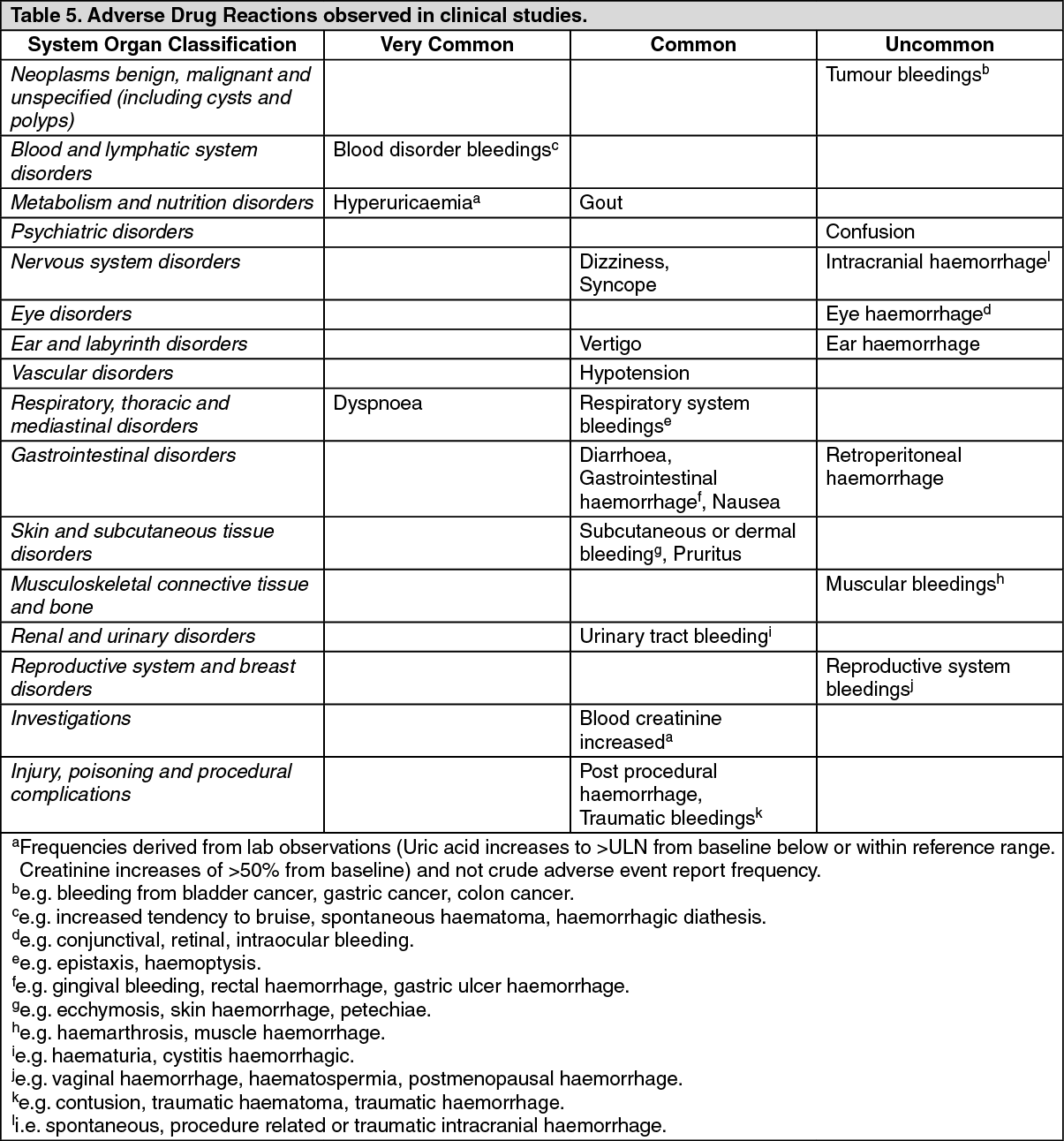
Tabulated list of adverse drug reactions: Adverse drug reactions from clinical studies with BRILINTA are listed by MedDRA System Organ Class (SOC) and frequency category determined by PEGASUS and PLATO trials in Table 5. Within each SOC and frequency category, adverse drug reactions are presented in order of decreasing seriousness. Frequency categories are defined according to the following conventions: Very common (≥1/10), Common (≥1/100 to <1/10), Uncommon (≥1/1,000 to <1/100), Rare (≥1/10,000 to <1/1,000), Very rare (<1/10,000), Not known (cannot be estimated from the available data). (See Table 5.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imagePostmarketing experience: The following adverse reactions have been identified during post-approval use of BRILINTA. Because these reactions are reported voluntarily from a population of an unknown size, it is not always possible to reliably estimate their frequency.
Immune system disorders: Hypersensitivity reactions including angioedema (see Contraindications).
Skin and subcutaneous tissue disorders: Urticaria, rash.
Blood disorders: Thrombotic Thrombocytopenic Purpura (see Precautions).
Cardiac disorders: Bradyarrhythmia, AV block (see Precautions).
Nervous system disorders: Central sleep apnoea including Cheyne-Stokes respiration (see Precautions).
View ADR Monitoring Form